Are you a Rushing Woman - and is it making your menopause harder?
She wakes before the alarm. Her to-do list is already running. She is capable, caring, competent — and quietly exhausted. Sound familiar? There's a name for it. And if you're heading into perimenopause in this state, the research suggests it matters more than most women realise.
The term "Rushing Woman's Syndrome" was coined in 2011 by Dr Libby Weaver, an Australasian nutritional biochemist with a PhD in biochemistry and decades of clinical experience. It describes a pattern she was seeing repeatedly in practice - women living in a state of relentless urgency, driven by packed schedules, high expectations of themselves, and an ever-present sense of not quite keeping up. It isn't a clinical diagnosis; it's a description of a modern epidemic. And its hormonal consequences, particularly as women move into their forties and beyond, are significant.
At its core, Rushing Woman's Syndrome describes what science calls sympathetic nervous system (SNS) dominance — the state in which the body's "fight or flight" response is chronically activated, even without any genuine physical threat. The body cannot distinguish between a sabre-toothed tiger and a full inbox. Both trigger the same cascade.
When the sympathetic nervous system is persistently switched on, the adrenal glands respond by producing adrenaline and cortisol. In short bursts, this is useful — cortisol helps you get up in the morning, meet a deadline, respond to a crisis. The problem emerges when the system never fully switches off, and cortisol remains elevated day after day.
The stress–hormone cascade
Step 1
Chronic rushing / perceived pressure
SNS dominance activated. Adrenaline signals "danger" to every cell
Step 2
Cortisol rises
Adrenal glands prioritise cortisol production. Progesterone and oestrogen take a back seat
Step 3
Sex hormone disruption
Sleep, mood, weight, libido and cycle regularity are all affected downstream
One of the key hormonal casualties of this state is progesterone. The adrenal glands produce both stress hormones and small amounts of progesterone but when they are overwhelmed by the demands of cortisol production, progesterone falls away. This matters because progesterone is far more than a reproductive hormone. It is calming, anti-anxiety, mildly anti-depressant, and helps regulate fluid balance and sleep. When it drops, women often notice a cluster of symptoms that can be easy to attribute to personality or circumstance: irritability, poor sleep, fluid retention, anxiety that seems to come from nowhere.
“Progesterone production takes a back seat when the body prioritises stress hormone production. And that matters — not just for reproduction, but for mood, fluid retention, weight balance, sleep and emotional stability.
”
Why menopause changes everything
Now layer the menopausal transition onto this picture. Perimenopause — which can begin in the early-to-mid forties and last anywhere from two to eight years — is characterised by fluctuating and then declining oestrogen and progesterone. Research published in Frontiers in Global Women's Health (2021) confirms that as oestrogen and progesterone decline, cortisol levels tend to rise — the HPG (reproductive) axis and the HPA (stress) axis are deeply intertwined, and changes in one directly influence the other.
This creates a compounding effect. The woman who has been running on adrenaline for twenty years arrives at perimenopause with adrenal glands that are already stretched, progesterone that is already low, and a nervous system that has forgotten what rest feels like. When her ovaries begin to reduce their output, there is less hormonal buffering available. Stress that once felt manageable begins to feel overwhelming. Symptoms that might have been mild become severe.
Declining oestrogen and progesterone weaken the body's natural buffering of cortisol, creating cycles of stress and symptom intensification. The result, as one researcher describes it, is a feedback loop: fluctuating hormone levels lead to symptoms, those symptoms increase stress, and that heightened stress in turn exacerbates the very symptoms driving it.
Research also points to a specific mechanism worth understanding. During perimenopause, the adrenal glands take over some of the production of oestrogen. If those same adrenal glands are already busy manufacturing stress hormones, they may have less capacity to make oestrogen and progesterone. In practical terms: the woman who cannot slow down may be compounding her own hormonal depletion.
What does Chinese medicine see?
This intersection of chronic stress and hormonal transition is not new to Chinese medicine — it has simply been described in different language for centuries. In classical TCM, the menopausal transition is understood as a natural shift in the balance of Kidney Yin and Yang, with the Liver and Heart often becoming disturbed when that foundation is insufficient to support them.
The pattern we might call "Rushing Woman's Syndrome" maps closely onto what Chinese medicine recognises as Liver Qi stagnation with underlying Kidney and Heart deficiency — a picture characterised by frustration, poor sleep, heat sensations, anxiety, and a sense of being stretched beyond one's limits. Treatment focuses not just on managing individual symptoms, but on supporting the underlying reserves that have been chronically taxed.
What does the research say about Chinese medicine and menopause?
Several areas of Chinese medicine research are relevant here, particularly for the symptoms most commonly worsened by chronic stress: hot flushes, sleep disruption, and anxiety.
Hot flushes and vasomotor symptoms
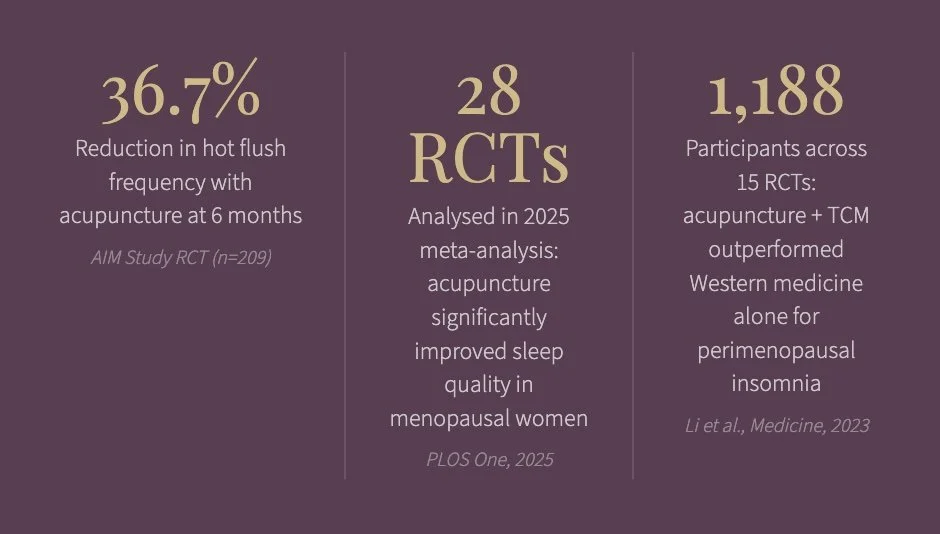
Acupuncture is one of the most studied TCM interventions for menopausal symptoms, particularly vasomotor symptoms. A large umbrella systematic review concluded that acupuncture provides a moderate reduction in hot flash frequency and improvements in health-related quality of life. A well-designed pragmatic randomised controlled trial, the AIM Study, found that vasomotor symptom frequency declined by 36.7% at six months in the acupuncture group, compared with an increase of 6.0% in the control group. The reduction was largely maintained at 12 months post-treatment, and only three women reported any adverse effects.
Research also suggests that acupuncture appears to influence cortisol, cortisol metabolites, and DHEA levels — and since cortisol tends to increase following menopause and contributes to changes in mood, metabolism, and bone density, it is possible that the same underlying mechanisms play a role in the treatment of hot flushes, depression, anxiety, sleep disorders, and abdominal weight gain.
Sleep disturbance
Sleep disruption is one of the most consistent complaints in perimenopausal women — and one of the most direct consequences of elevated cortisol and low progesterone. A 2025 systematic review and meta-analysis published in PLOS One (28 RCTs, reviewed to April 2024) found that acupuncture significantly lowered Pittsburgh Sleep Quality Index scores, increased total sleep time and sleep efficiency, and reduced time awake after sleep onset. The effect was maintained at four-week follow-up.
A 2023 meta-analysis of 15 RCTs involving 1,188 patients found that acupuncture combined with Chinese herbal medicine was more effective than Western medicine alone for perimenopausal insomnia, with improvements in sleep quality scores and a significant reduction in anxiety scores.
Mood and anxiety
The experience of anxiety and mood disturbance during perimenopause is often attributed to "hormones" but as we've explored, the stress layer matters too. Acupuncture research for anxiety in peri and post-menopausal women shows consistently positive results across multiple controlled trials, and the combination of acupuncture and medication - either Chinese or Western has been found to regulate neuroendocrine function, improve sleep quality, and reduce levels of anxiety and depression.
It's important to note that these findings come from studies of varying methodological quality, and the evidence base continues to develop. Chinese medicine is not a replacement for conventional assessment and care, particularly where anxiety is severe or mood disturbance is significantly affecting function.
The most important thing to understand
If you are a Rushing Woman heading into perimenopause, the most significant thing Chinese medicine can offer may not be a needle or a herb - it is the lens through which your whole picture is understood. Your symptoms are not separate problems to be managed in isolation. They are signals from a system that has been running hard for a long time, and that now has less in reserve to cushion the transition.
The research on acupuncture and Chinese herbal medicine suggests genuine benefit for the symptoms most commonly reported by perimenopausal women. But the deeper message of both Dr Libby Weaver's work and the classical Chinese medical tradition is the same: the body cannot heal from a state of perpetual urgency. Part of the treatment is permission — and practical support — to slow down.
Ready to understand your menopause picture more clearly?
A consultation at Emerald Acupuncture & Chinese Medicine includes a full intake of your health history, cycle pattern, sleep, digestion, and emotional landscape — so that care is tailored to you, not a protocol.
Regulatory disclosure
This blog post is for general educational purposes only. It does not constitute medical or health advice and should not replace professional medical assessment or treatment. Individual responses to Chinese medicine vary and outcomes cannot be predicted or guaranteed. The research cited represents published peer-reviewed literature; it does not imply that these results will be achieved in any individual case. Sandra Cant is an AHPRA-registered acupuncturist and Chinese medicine practitioner. This content has been prepared in accordance with the Health Practitioner Regulation National Law advertising requirements. No testimonials are included. If you are experiencing distressing perimenopausal or menopausal symptoms, please speak with your GP or a qualified women's health specialist.
Key references
Weaver L. (2011, updated 2023). Rushing Woman's Syndrome. Hay House.
Dinforming Science Institute (2021). Steroid hormone secretion over the course of the perimenopause: Findings from the Swiss Perimenopause Study. Frontiers in Global Women's Health, 2, 774308.
Winona Health (2024). The relation between cortisol and menopause. Based on Seattle Midlife Women's Health Study data.
Avis NE et al. (2016). Acupuncture in menopause (AIM) study: a pragmatic, randomized controlled trial. Menopause, 23(6), 626–637. PMC4874921.
Xu M et al. (2025). Acupuncture as an independent or adjuvant therapy for menopausal insomnia: a systematic review and meta-analysis. PLOS One. doi:10.1371/journal.pone.0318562.
Li Z et al. (2023). Acupuncture combined with Chinese herbal medicine in the treatment of perimenopausal insomnia: a systematic review and meta-analysis. Medicine, 102(45), e35942.
Befus D et al. (2018). Menopausal hot flashes and acupuncture: a scoping literature review. Menopause.
Evidence Based Acupuncture (2023). Acupuncture treatment for menopausal symptoms. evidencebasedacupuncture.org.